

Stings Like a Bee
Author: Noopur Basu MD
Peer-Reviewer: Kareem Shahin DO
Final Editor: Katherine Boehm, DO, Will Denq, MD, CAQ-SM
A 16 year old male presents to the ED with complaints of right upper extremity weakness, pain, and paresthesias after falling and striking his head during a football game. No loss of consciousness.
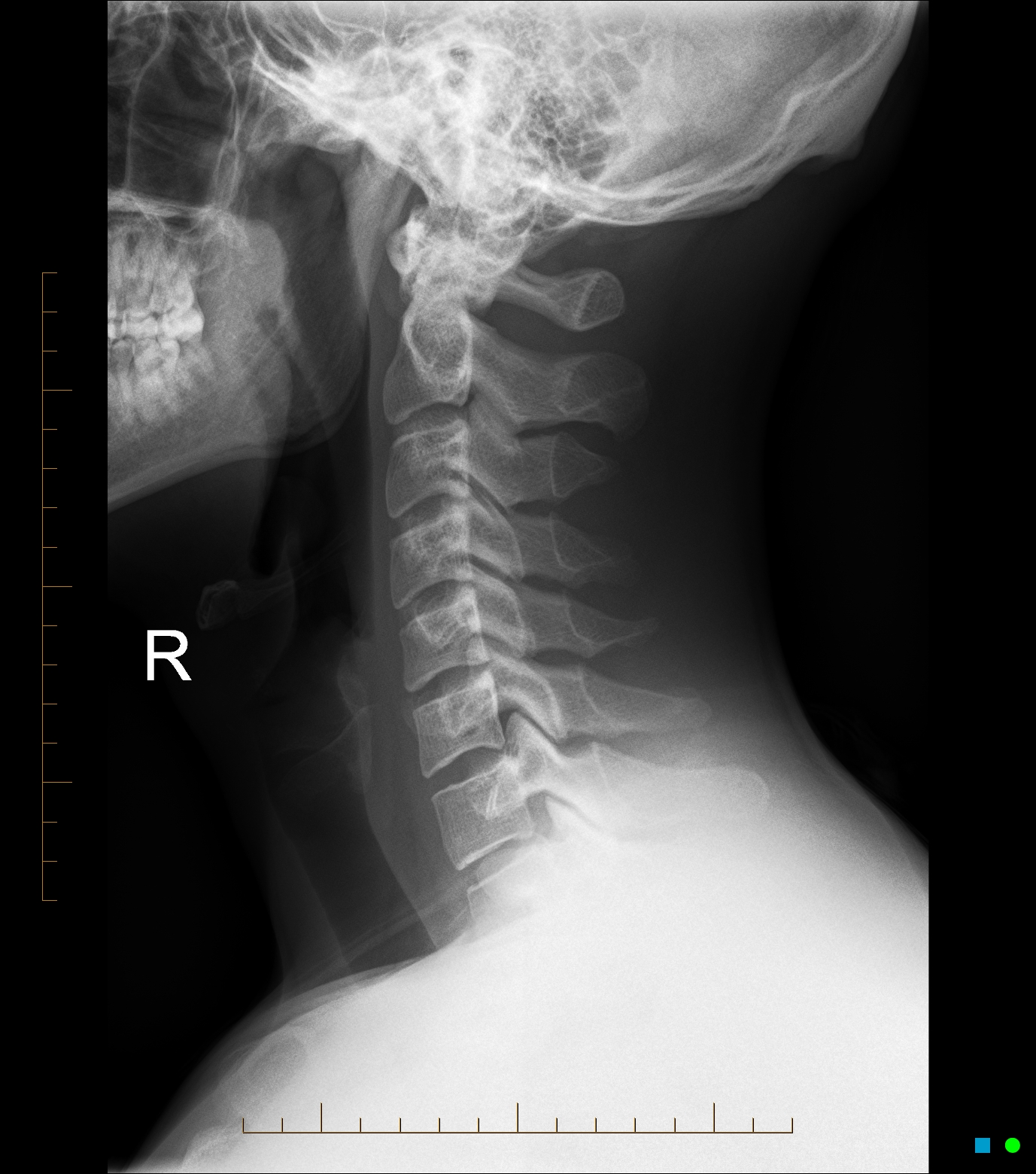
Image 1. Lateral cervical radiograph. Case courtesy of Andrew Dixon, Radiopaedia.org, rID: 32505
What is the mechanism of injury?
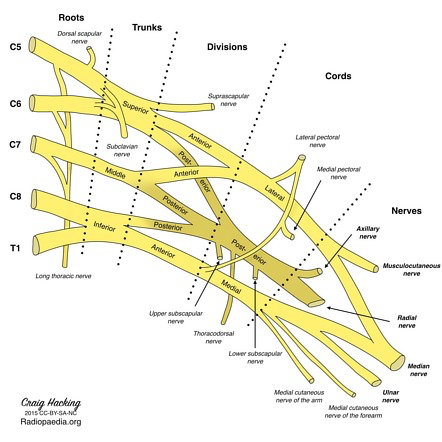
There are three possible mechanisms of injury: traction injury from stretch, percussive injury from a direct blow, or neck hyperextension with ipsilateral flexion causing direct nerve compression [1-6]. See Image 2 for a brief and traumatizing reminder of the brachial plexus.
References
[1] Thein L. Rehabilitation in shoulder injuries. In: Rehabilitation Techniques in Sports Medicine, 2nd ed, Prentice WE (Ed), Mosby-Year Book, Inc, St. Louis 1994. no abstract available
[2] Sallis RE, Jones K, Knopp W. Burners: offensive strategy for an underreported injury Phys Sportsmed. 1992;20:47.
[3] Hershman EB. Injuries to the brachial plexus. In: Athletic Injuries to the Head, Neck, and Face, 2nd ed, Torg JS (Ed), Mosby-Year Book, St. Louis, MO 1991.
[4] Benedetto M, Markey K. Electrodiagnostic localization of traumatic upper trunk brachial plexopathy. D Arch Phys Med Rehabil. 1984;65(1):15.
[5] Markey KL, Di Benedetto M, Curl WW. Upper trunk brachial plexopathy. The stinger syndrome. Am J Sports Med. 1993;21(5):650.
[6] Watkins RG . Neck injuries in football players. Clin Sports Med. 1986;5(2):215.
[7] Schroeder GD, Vaccaro AR. Cervical Spine Injuries in the Athlete. J Am Acad Orthop Surg. 2016 Sep;24(9):e122-33. doi: 10.5435/JAAOS-D-15-00716. PMID: 27479833.
[8] Rihn JA, Anderson DT, Lamb K, Deluca PF, Bata A, Marchetto PA, Neves N, Vaccaro AR. Cervical spine injuries in American football. Sports Med. 2009;39(9):697-708. doi: 10.2165/11315190-000000000-