

You’re Driving Knee Crazy
Author: Madeleine Birch, MD
Peer-Reviewer: Mark Hopkins, MD
Final Editor: Alex Tomesch, MD, CAQ-SM
A 70 year old female presents with knee pain after high speed MVC. Patient felt a “pop” in her knee as it made contact with the dashboard. The “pop” was followed by severe pain and inability to move her right knee. She is tender over her right knee with obvious deformity.


Image 1: Obvious deformity to knee joint upon initial presentation. Image by Mark Hopkins, MD
Image 2: Plain lateral x-ray of right knee [1]
What is the difference with artificial joints?
Knee subluxation in artificial joints is uncommon (reported 15 subluxations in more than 3000 primary total knee arthroplasties), but can more easily occur without overt trauma [9]. Posterior subluxations in artificial joints is more common than anterior and is usually associated with ACL and PCL sacrificing surgeries, poor tibial component alignment and pre-existing neurological disorders [9]. As they are less traumatic, they may have fewer concomitant injuries, but keep a high index of suspicion.

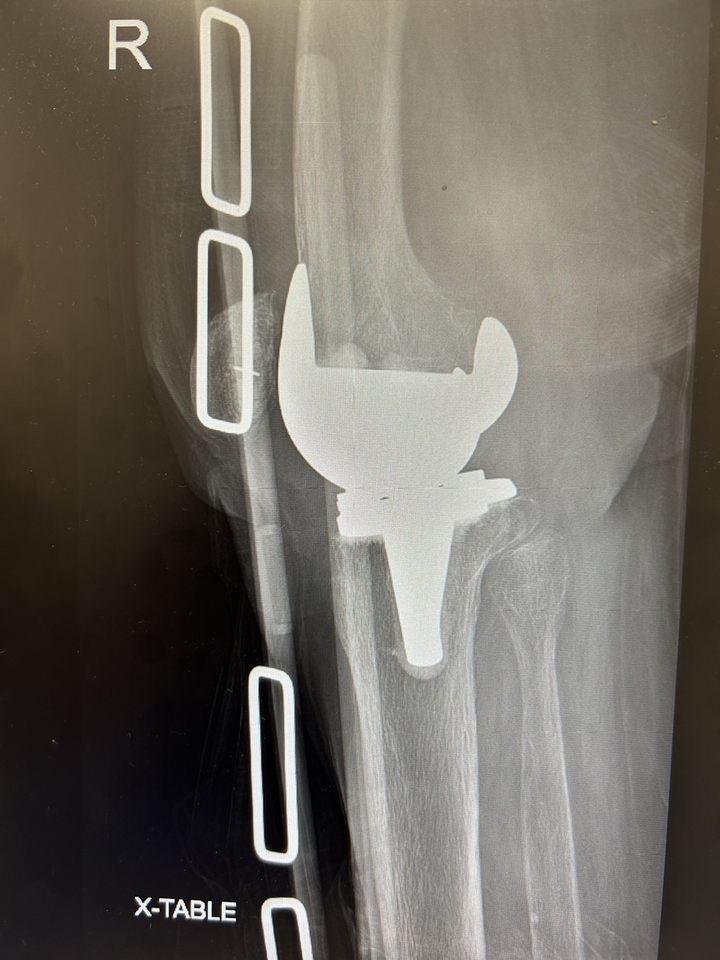
Images 3 and 4, x-ray of posterior subluxation and post-reduction film of prosthetic joint. Courtesy of Mark Hopkins, MD
References
[1] Duprey K, Lin M (February 2010). "Posterior knee dislocation". The Western Journal of Emergency Medicine. 11 (1): 103–4. PMC 2850837. PMID 20411095.
[2] Knipe, H., Murphy, A. Knee dislocation. Reference article, Radiopaedia.org. (accessed on 24 Oct 2022) https://doi.org/10.53347/rID-42748 DOI: https://doi.org/10.53347/rID-42748 https://radiopaedia.org/articles/42748 rID: 42748
[3] Fanelli GC. Knee Dislocation and Multiple Ligament Injuries of the Knee. Sports Med Arthrosc Rev. 2018 Dec;26(4):150-152. doi: 10.1097/JSA.0000000000000220. PMID: 30395055.
[4] Karkos CD, Koudounas G, Giagtzidis IT, Mitka MA, Pliatsios I, Papazoglou KO. Traumatic Knee Dislocation and Popliteal Artery Injury: A Case Series. Ann Vasc Surg. 2018 Jul;50:298.e13-298.e16. doi: 10.1016/j.avsg.2018.01.084. Epub 2018 Mar 5. PMID: 29518501.
[5] Mohseni M, Simon LV. Knee Dislocation. [Updated 2022 Jul 18]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470595/ PMID: 29262122
[6] Gottlieb M, Koyfman A, Long B. Evaluation and Management of Knee Dislocation in the Emergency Department. J Emerg Med. 2019 Nov 8:S0736-4679(19)30826-1. doi: 10.1016/j.jemermed.2019.09.042. Epub ahead of print. PMID: 31711826.
[7] Natsuhara KM, Yeranosian MG, Cohen JR, Wang JC, McAllister DR, Petrigliano FA. What is the frequency of vascular injury after knee dislocation? Clin Orthop Relat Res. 2014 Sep;472(9):2615-20. doi: 10.1007/s11999-014-3566-1. PMID: 24658901; PMCID: PMC4117920.
[8] Kupczik F, Schiavon MEG, Vieira LA, Tenius DP, Fávaro RC. Knee Dislocation: Descriptive Study of Injuries. Rev Bras Ortop. 2013 Jun 20;48(2):145-151. doi: 10.1016/j.rboe.2012.10.002. PMID: 31211120; PMCID: PMC6565857.
[9] Aderinto J, Gross AW, Rittenhouse B. Non-traumatic anterior dislocation of a total knee replacement associated with neurovascular injury. Ann R Coll Surg Engl. 2009 Nov;91(8):658-9. doi: 10.1308/003588409X432509. Epub 2009 Aug 14. PMID: 19686618; PMCID: PMC2966241.