
My Bladder, My Back
Author: William Denq, MD, CAQ-SM
Peer-Reviewer and Final Editor: Alex Tomesch, MD, CAQ-SM
68 year old male PMH significant for diabetes, spinal arthritis, and recurrent urinary tract infections presents to the Emergency Department with 5 weeks of dysuria and low flank pain. He reports subjective fevers and chills, but denies nausea, vomiting, or trauma. Plain films of the lumbar spine were obtained (Image 1).
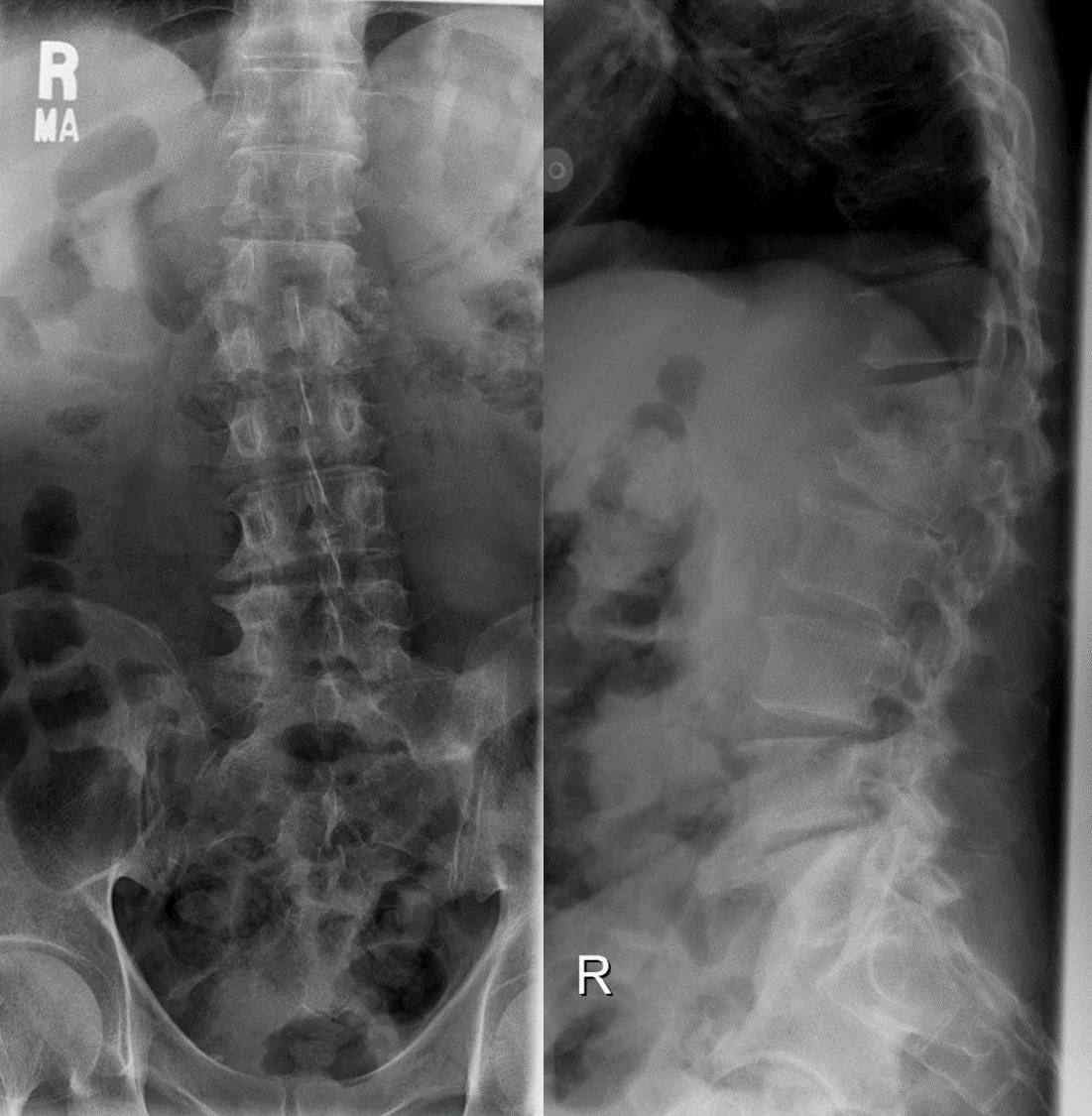
Image 1. Plain radiograph of the lumbar spine, anteroposterior (left) and lateral (right). Image courtesy of Matt Skalski, Radiopaedia.org, rID: 25127
What is the most likely diagnosis?
Spondyolodiscitis. This heterogenous term spans vertebral osteomyelitis, spondylitis, and discitis [1]. See Image 2 for the annotated plain film.

Image 2. Loss of T12-L1 disc space with destruction and collapse of adjacent vertebral bodies. Plain radiograph of the lumbar spine, lateral. Annotation by author. Image courtesy of Matt Skalski, Radiopaedia.org, rID: 25127
References
[1] Herren C, Jung N, Pishnamaz M, Breuninger M, Siewe J, Sobottke R. Spondylodiscitis: Diagnosis and treatment options - A systematic review. Dtsch Arztebl Int. 2017;114(51-52
[2] :875-882. doi:10.3238/arztebl.2017.0875
[3] Gouliouris T, Aliyu SH, Brown NM. Spondylodiscitis: update on diagnosis and management. J Antimicrob Chemother. 2010;65 Suppl 3:iii11-iii24. doi:10.1093/jac/dkq303
[4] Amini MH, Salzman GA. Infectious spondylodiscitis: diagnosis and treatment [published correction appears in Mo Med. 2013 Mar-Apr;110(2):121] [published correction appears in Mo Med. 2013 Mar-Apr;110(2):121]. Mo Med. 2013;110(1):80-84.
[5] Raghavan M, Lazzeri E, Palestro CJ. Imaging of Spondylodiscitis. Semin Nucl Med. 2018;48(2):131-147. doi:10.1053/j.semnuclmed.2017.
[6] Berbari EF, Kanj SS, Kowalski TJ, et al. Infectious Diseases Society of America (IDSA): clinical practice for the diagnosis and therapy of native vertebral osteomyelitis in adults. Clin Infect Dis. 2015;61:26–46.